Equine
Reproduction
Dr.
Jack Sales, DVM
CopyrightÓ2004
Lesson Eight
Neonatal Management and Common Neonatal Diseases
Including Orphan Foal Management and Management During the First Six Months.
Assignment:
Chapter 11 in the text.
In this lesson we will discuss all the important managerial aspects of new born foal management as well as orphan foal management, and follow the foal to six months of age. There are some critical things that need immediate attention after a foal is born. This will help prevent complications following delivery of a live foal.

I.
Immediate
newborn management.
A.
Make sure amnion sac is not covering foal’s
muzzle and restricting breathing.
B.
It is important for last transfer of blood from
mare to foal prior to breaking of the cord.
C.
The foaling environment must be clean with
good footing. (wood shavings or sawdust
base
covered with clean, dry straw.
 D. Foal
should be bright and alert from beginning.
D. Foal
should be bright and alert from beginning.
a.
Clear breathing passages.
b. Allow mare and foal to
bond.
c. Foal should stand within
first hour. (The foal
will
usually attempt to stand
within 10 to 15 minutes
of foaling.)
 d. The foal
should nurse within
d. The foal
should nurse within
the first 2 hours. (Foal will
usually attempt to nurse within
first half hour.)
e. Naval should be dipped in a
disinfectant (nolvasan
(chlorhexidine) or
betadine (tamed
iodine) usually as soon as
possible
after the cord breaks.
 f. Using an enema on the foal is
f. Using an enema on the foal is
advisable. Normally done
anytime
after the foal has been up
and
nursing.
g. If mare hasn’t been vaccinated for
tetanus within the last
few months
of pregnancy, the foal
should be
administered a tetanus
antitoxin.
Common problems
must be recognized and dealt with effectively if they arise in the first few
days of a foal’s life.
II. Problems
associated with the immediate post foaling period.
A. Meconium (first manure) impaction.
1. Straining to pass manure or signs of colic may indicate
meconium impaction.
2. Enema (standard or mineral oil fleet enema) is preventative
as well as a treatment for this condition.
B. Patent urachus – leakage of urine from the umbilical cord
when straining to urinate.
1. Strong Iodine (7%) application to naval every 6 hours until
closure. Sometimes requires veterinary attention or use of stronger drying
agent (silver nitrate application).
C. Ruptured urinary bladder.
1. Appears normal for first 24 hours.
2. The abdomen begins filling up with urine which causes the
belly to enlarge and the foal to become weak and depressed.
3. Requires surgical correction.
D. Neonatal malajustment syndrome or
“dummy foal”
1. These foals may be normal at birth and become “dummy” on
the second or third day after birth. (Foals stop nursing, walk around stall as
if blind.)
2. Usually associated with systemic infection (septicemia) or
possible loss of blood to brain early in life.
E. Septicemia
1. Possible fever, lack of nursing reflex, weak, depressed
foals from birth.
2. Systemic infection contracted within the womb.
F. Failure of passive transfer of antibodies.
1. Lack of colostrums intake during first 12 to 24 hours of
birth.
1. Mare dies at birth.
2. Mare leaks out colostrums prior to birth.
3. Mare has inadequate levels of colostrums.
4. Foal does not nurse properly for first 24 hours. There is
no placental transfer of antibodies to foal. The only way a foal can naturally
obtain neonatal protecting antibodies is through colostrums intake.
2. Blood analysis after 18 hours of life to
detect IGG antibody levels.
1. 400mg/dl is considered partial failure of passive transfer
and requires IGG rich plasma transfusion to prevent infection problems during
the first few months of life.
a. 400 – 800mg/dl. Most of these
foals will survive,
 but an IGG
rich plasma transfusion would probably
but an IGG
rich plasma transfusion would probably
be
beneficial.
b. 800mg/dl.
This level of antibody transfer is
considered
adequate and ideal and will provide the
young foal
with adequate protective antibodies for
good health
until natural antibodies are developed
at 3 to 4
months of age.
III. The raising of
an orphan foal is sometimes necessary.
Care of the
orphan foal.
A. An orphan foal is any foal whose dam is unable to
provide adequate nourishment
through normal nursing.
B. Immediate care consists of
making sure the foal is able to consume colostrums
during the first 12 hours of
birth. (If the dam cannot supply this, use of colostrums
from another mare is
needed). If colostrums are not
available, Plasma rich IGG
antibodies should be given to
the foal by stomach tube in the first 12 to 24 hours
of life, or intravenously
shortly thereafter.
Meeting the needs of the growing orphan foal.
A. Nurse mare.
1. The mare must accept
orphan foal. (Urine or manure of mare can be rubbed
on the foal).
2. The mare must be a
good milker.
3. Initial nursing must
be attended.
B. Goats have been used
successfully to raise an orphan foal.
C.
Hand feeding
1. Milk replacer (quick
formula is evaporated can milk and water in equal
proportions)
Commercial – Foal Lac.
 2. Use of a lamb’s nipple is
best.
2. Use of a lamb’s nipple is
best.
3. First week: feed every hour. Second week
feed every 2 hours.
Third week feed every 3
hours. Third week feed every 3 hours.
Fourth week feed
every 4 hours. Thereafter
feed 4 times per day.
4. Attempt to switch to bucket feeding as
soon as
possible.

Behavior
of orphan foals
A.
Orphans should be around a gentle horse or pony to allow him/her to
become
a “horse”.
B. The sooner they are exposed to
other weanlings the better.
C. Don’t encourage or tolerate development of
bad habits around humans (nipping,
kicking, rearing). Although cute in the young
foal, this behavior is dangerous
when coming from a growing
horse.
IV. Factors to be considered during the first 6 months of a
foal’s life.
Six months of age is the most common
age for weaning. (The permanent removal of foal from dam so no more nourishment
is derived from the dam.)
A. The first 6 months.
1. Exercise and exposure to the outdoors
is important once the foal is
found to be healthy
and sound.
2. Early handling – if
various forms of restraint and handling are calmly
introduced during the suckling
period, the foal should be very tractable
by the time it is
weaned.
3.
Foal imprinting – the development of the human-horse bond shortly
after birth.
a.
Haltering, leading, handling the legs.
 4.
Nutrition: creep feeding of the foal should
4.
Nutrition: creep feeding of the foal should
begin as soon as practical. At
least by
the third month
of life.
a. Protein requirements of creep
feed 16-18%
b. Ca:P ratio 1.2 to
2 : 1
c. Lysine (good quality protein) is
important part of quality creep feed.
5. Worming and
vaccinations.
a. Deworm every 2 months during first year of
life.
Rotate strongid
with a benzimidazole at 2, 4 and 6 months.
At 8 months start ivermectin.

b. EEE, WEE,
and
tetanus at 2 months with a booster 3 to 4 weeks later.
At
6 months flu and rhino and possibly strangles. Other
vaccines depending on area of the country. (Rabies,
horse fever, equine protozoal myeloencephalitis,
lyme disease,
botulism.)

6. Suckling stage
diseases.
a. Foal heat scours (diarrhea).
1.
Normally is eliminated when mare goes out of heat.
2.
Two ounce of Pepto Bismol can be helpful every 6 hours.
b.
Infectious diarrhea.
1.
Can be serious. Foals dehydrate easily. Usually need
veterinary attention.
c. Stomach and intestinal ulcers.
1.
Seem to be caused by stress.
2. Excessive salivation, grinding teeth,
diarrhea.
aa.
Mylanta or Maalox is helpful.
bb.
Anti-ulcer medication can be effective.
cc.
(Prevents secretion of stomach acids).
d.
Infectious Pneumonia
1.
Normally requires veterinary care.
2.
Rodococcus pneumonia (bacterial pneumonia – dust
pneumonia) 2-6 months of age, coughing.
Abscesses
in the lungs.
e.
Umbilical hernia
1. If small, may close on its own by 6 months.
2. Require surgical closure if large or if not
gone
by 6 months.
f. Navel
through the umbilical cord shortly after birth. (This is why
disinfectant
application to cord is important).
1. Spreads to joints and causes severe
infections usually causing permanent joint disability.
2. Requires extensive veterinary treatment for
chance of future usefulness.

g.
Crooked limbs
1. Usually medial deviation of the knees.
2. May require surgery to correct.
3. Pereosteal stripping
and or stapling of the distal
radial epiphysis.
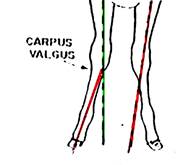
Green lines demonstrate correct
conformation.
Red lines illustrate angular deformity.
h. Contracted tendons
1. Seen to knuckle over at the fetlock. superficial digital
flexor contraction or development of a club foot with
inability
to put heel on the ground. (Deep digital
flexor contraction).
2. Surgery to cut offending tendon may
be necessary.

Contracted
tendon and
club foot
B. Weaning
1. Normally done at 6 months of age. Possible as
early as 4 months.
2.
Group weanlings together and allow them to have visual contact
with mothers.
3. Have
good, safe fencing between weanlings and mares.
4. Alternate approach is complete separation
from sight and hearing.
This is more stressful to the foal.