Equine Health
and Disease Management
By
Dr.
Jack Sales, DVM
Copyright © July 2003

As we study Equine Health and Disease
management in this course we will want to become familiar with the internal
anatomy and functions of the horse as well as the external anatomy and
functional parts of the body. In each section, become familiar with the area on
the horse’s body that is involved in the disease process. This will make it
much easier to understand and remember.
Lesson 1
Musculoskeletal System
The first system we are going to study
is the musculo-skeletal system. This will include the
main muscles and major bones of the body, with emphasis on the lower limbs. It
is important to realize the front limbs of the horse carry the majority of the
weight of the horse. The front limbs carry approximately 65 to 70% of the
horse’s weight when standing and, at times, even more when in motion. For this
reason we will find that the front limbs are the ones that seem to have more
lameness problems in the average horse. Of course, depending on the use of the
horse, there are times in which the hind legs are used more extensively, and in
these cases we see a number of hind limb problems. Think of the reining horse
and how much pressure is put on the hind limbs during different maneuvers.
In order to study the lameness
conditions of the front and hind limbs, it is important the student have some
knowledge of equine anatomy. As we study
the different problems of the front and hind limbs, we will be referring to
limb anatomy. It will be necessary for
you to become familiar with the terms used as we study the particular area of
the leg. There will be diagrams of limb anatomy throughout our discussions of
lower limb lameness. It is important that as we identify some of the lameness
problems of the front and hind limbs, you can relate each problem to the area
of the anatomy that is affected.
When dealing with lameness problems in
the horse, it is important that we categorize each lameness problem as either acute, meaning that it was a sudden lameness that came on
very rapidly, or chronic, which would indicate a
problem or lameness that had a gradual and usually progressive onset. For
example, a sudden bone break or fracture would be considered an acute lameness
whereas a condition such as ringbone is considered a chronic condition that comes
on gradually over a period of months or years, and usually continues to get
worse and worse.

Let’s start our study of lameness
problems in the horse with the shoulder area of the horse’s front limb, and
then continue downward toward the hoof. One thing to keep in mind regarding
lameness in the horse is that most lameness is going to be seen in the lower
limb area, from the knee down. But for
continuity, we will start our study of front limb lameness in the shoulder.
Shoulder Sweeny
This is a condition of the shoulder that is
characterized by atrophy (loss of muscle mass) over the shoulder blade. The
muscles over the scapula will atrophy (shrink or disappear) due to an injury to
the nerve that supplies these muscles. This nerve, the suprascapular nerve, is
usually injured by a blow to the area around the point of the shoulder, and if
the nerve is damaged severely enough, these muscles will lose the innervation
from that nerve and begin to waste away. This will usually cause a mild lameness
or funny way of going by the horse, but many times the horse will learn to
compensate for this muscle loss and can be used for his intended purpose.
Looking at a horse with shoulder sweeny,
you can easily tell that the shoulder on one side is not full in appearance,
and if you look closer, you can even see that the skin is just covering the
bone of the shoulder blade, with the spine of the scapula (the bony ridge of
the center of the shoulder blade) very prominent. This is usually a permanent
condition, in that this nerve, once damaged or severed, does not grow back.

Fracture of the Scapula
A fracture of the scapula or cracked scapula can
occasionally occur and is usually caused by as severe blow or kick over the
shoulder blade. All bone fractures show a sudden, usually severe lameness and
it is usually evident from severe swelling, where the fracture is located.
A horse that sustains a fracture of
the shoulder blade can usually be stall confined for a period if 3 to 6 months and healing will
usually be complete. Unless the bone break extends into the shoulder joint
area, the horse will normally heal without further lameness. A concept that you should keep in mind about fractures
or broken bones is that any break that extends into a joint area will have the
potential of causing a future arthritis of the affected joint after healing
occurs. So any fracture that extends into a joint area, unless surgically
plated or pinned by a veterinarian, will usually heal with continued future
lameness in that horse because of the arthritis in that particular joint.
Bicipital Bursitis
This is a condition that causes a lameness of the
shoulder area. The bicipital bursa is found on the front of the shoulder joint,
and when there is a blow to this area or there is a strain to this area, the
horse will show a short stride in the affected shoulder. You can usually make
the horse flinch to pressure directly over the point of the shoulder from the
front. Also if you pick up and extend the shoulder, the horse may elicit a pain
response.
Anti-inflammatory
therapy (refer to the upper and lower leg therapy section in this lesson) is
helpful for this problem, and if severe, a veterinarian can administer local
injections ( refer to Injectable therapy in lesson 2)
to help resolve the problem.
Fracture of the humerus
A bone break of the humerus is a very serious
injury. Oftentimes it is considered a life threatening injury.
Because the horse has numerous large
bones making up the front and hind limbs, we will talk about fractures of the
major bones of the horse’s limbs as a general subject.
All that will be discussed on this
subject applies to all the major bones of the horse’s limbs. The following is a
summary of most major bone fractures in the horse.
Fractures in the
Major bones of Horses
Fracture = Broken Bone = Broken Leg
Types Of Fractures
n Simple
Fractures
n No
displacement of bone ends.
n Only
one fracture line
n Compound
Fractures
n Broken
piece of bone breaks through skin
n More
serious because of introduction of infection.
n Comminuted
Fractures
n More
than one fracture line in a single bone.
n More
than two pieces of bone make up the fracture
Other Types of Fractures
n Compound
comminuted fractures
Most devastating
type
Most difficult to
repair with good outcome
n Incomplete Fractures
n Fracture
line doesn’t go all the way through bone
n Hairline
fractures
n Less
serious
n Usually
only show mild lameness
n Can
warm out of lameness
n Can
turn into devastating complete, compound, comminuted fracture if horse
continues work.
Prognosis (
Outcome)
n Large
bone fractures (Humerus,Radius,
Femur, Tibia).
n Very
serious, possibly life threatening
n Extreme
swelling, and pain
n Usually
poor outcome
n Medical
advances still lagging behind
n Fracture
lines extending into joint
n Secondary
arthritis very possible after complete healing
n Future
soundness unlikely
n Economics
n Great
expense involved in attempts to repair
n Horse’s
weight a factor
n Adult
horses weigh so much,
often will founder in opposite leg
n Horse’s
temperament a factor
n May
have to spend time in a sling
Osteochondritis Dissecans (OCD)
OCD is a disease condition in
the horse that can be found in nearly any major joint of the horse’s limbs.
We will discuss it here at the shoulder
joint and what you learn here will apply to OCD as seen in any other joint of
the front or hind limb.
OCD is a condition that is seen as it develops
in young growing horses. It is associated with the areas of growth of the long
bones and the long bones grow at the ends of the bones close to the joints.
Although the exact cause has not been determined, research indicates that
either a nutritional imbalance or a change in the rate of growth (too rapid
growth) could be the main cause. An area in or around the joint loses blood
supply and the area necrosis (dies), which leaves bone chips, or cartilage
flaps or bone cysts (holes in the bone) in and around the joint. This causes
the horse joint pain, which leads to lameness, especially if the horse has
started into training.
X-rays are normally diagnostic to identify the
problem and arthroscopic surgery may be indicated to remove bone chips, spurs
or bone cysts. The success of the surgery is dependent on the amount of damage
and the length of time the condition has been there. Some horses respond to
treatment well, some never fully recover, developing a long-term joint
arthritis that will plague the horse for his lifetime.
Fractures of the Radius or Ulna
Refer
to fractures of major bones above
Hygroma of the Elbow (Capped Elbow
or Shoe Boil)
This is a condition caused by a
blow or irritation to the point of the elbow. Can often be seen in horse’s that
lay on hard ground with their elbows directly on the hard surface, or their
heel or heel of the shoe putting pressure on their point of the elbow. There is normally a swelling on the point of
the elbow that is slightly painful and full of fluid. It normally does not
cause lameness. This condition can become chronic where scar tissue is formed
over the elbow and it does not go away. In the acute case, a veterinarian can
be called out to drain and possibly inject the shoe boil, hopefully bringing
the swelling down The swelling may or may not return.
To prevent this from occurring in horses
prone to banging their elbow, a donut, which is a foam piece attached around
the pastern by Velcro or a buckle, provides a cushion which prevents the heel
from making contact with the point of the elbow.
Cellulitis
This condition can occur on the front or hind leg,
but I will discuss it here because it is commonly found in the forearm area. It
is an extensive infection usually caused by a puncture wound in the forearm
area. The puncture causes the infection to build and fester in the deep tissues
of the forearm and usually it will suddenly blow up (swell excessively)
overnight. It is hot to the touch and painful and usually causes a mild
lameness or tenderness of the leg.
If you can find the area of initial
penetration of the wound, make sure there is good drainage (sometimes the wound
is scabbed over and this traps the infection.)
Clean the area with disinfectant soap and
water and establish good drainage. The horse will need a tetanus booster and
normally your vet will recommend daily antibiotics until the infection is under
control.
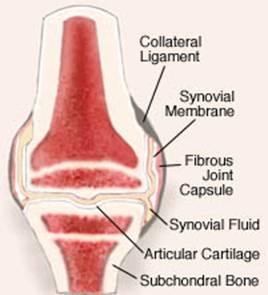
Degenerative Joint disease (DJD)
(Osteoarthritis)
This is a condition that can affect many
of the lower limb joints, and we will discuss it here as we begin to discuss
the carpus or knee of the horse. What we say here will apply to other joint
areas of the horse’s limb that are affected by DJD.
DJD as associated with the knee joint of
the horse refers to the every day wear and tear that joints undergo, eventually
resulting in mild to severe arthritic changes within a joint. We are normally
talking about older horses when we talk about DJD, but it is important to
realize that this wear and tear starts early in the athletic horse’s career and
minor sprains and strains of joints in the early years can result in the start
of DJD. The problem may become severe
enough to end the young horse’s career.
Small chips in the knee joints can be
removed arthroscopically and the horse will normally recover to compete another
day, but the damage that is done is never fully healed and eventually more
joint damage occurs which becomes additive.
This process of additive repeated damage to the joints is what is
referred to as DJD in all its stages. Refer to anti-inflammatory therapy and
lower leg therapy for details on treatment of the different stages of DJD.
Hygroma of the carpus
A blow to the front of the knee can occasionally
occur that can cause a large fluid filled swelling on the surface of the knee.
It is usually not painful, but can be unsightly and cause a restriction of knee
movement. It is necessary to contact a Veterinarian who will normally drain the
fluid off and inject with an appropriate anti-inflammatory medication and
recommend that the horse be stall confined with pressure wraps over the knee
until the skin attaches smoothly over the front of the knee.
If
exercise continues, the fluid will usually build back up due to action of the
knee.
Epiphysitis
This is a condition seen in the
young growing horse usually between six months and 2 years of age. Although it
can be seen in the knee, ankle (fetlock), or hock areas, it is normally a
problem in the knee area. The distal radial epiphysis (directly above the knee
joint) becomes inflamed due to imbalanced nutrition or excessively rapid growth
spurts. There can be some mild lameness.
There is normally an enlargement of the
area involved. This must be corrected by balancing the diet and/or slowing the
growth rate by cutting back on energy feeds such as grain and supplements. It is wise to notify a veterinarian to help
you manage this condition so no permanent growth abnormalities occur at the
epiphysis.
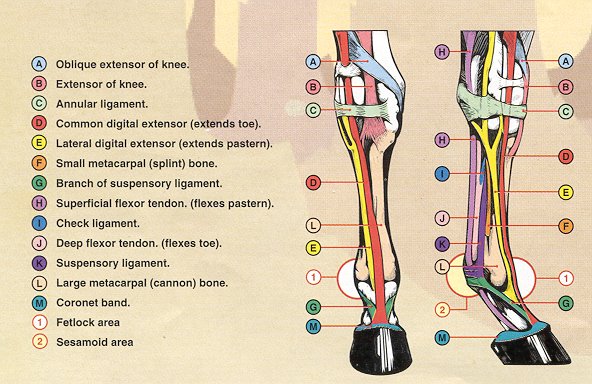
Moving
down to below the knee we should keep in mind that the anatomy in this area
should be very familiar to us. If we are not knowledgeable of this lower limb
anatomy please take some time to become very familiar with it. From the knee
down, the anatomical structures are the same as from the hock down. There is no
muscle found below the knee or below the hock. It should also be kept in mind
that the blood supply to the tissues and bone structure below the knee and hock
is not very good which means that healing of wounds or injuries is not very
good either.
Bucked Shins (Shin
Bucked)
This condition is seen in young horses in early
training, especially race training. The shin or cannon bone undergoes slow
strengthening as the horse gets heavier and heavier into training, adapting to
the extra concussion it is exposed to during this training process. Sometimes
the training can get ahead of the strengthening of the cannon bone and soreness
and inflammation of the front of the cannon bone occurs. The horse will be sore
to the touch, and heat and some swelling may be evident on the front of the
shins. This usually shows up initially as an acute condition, but if it is not
resolved it can turn into a continuous or chronic condition plaguing the horse
during much of his early career.
Therapy to relieve the heat, pain and swelling
is in order (refer to lower leg therapies) and controlled exercise is also
important to allow the cannon bone strength to catch up with the training
regime.
Splints
This is a similar condition
seen in young horses in training, and is caused by a strain of the ligament
that attached the splint bone to the cannon bone. The splint is usually seen
high on the cannon bone between the attachment of the splint bone and the
cannon bone on the side of the leg (inside or outside). It is painful when
pressed on and usually warm to the touch. Some firm swelling will also usually
be found. As this splint heals, calcium will fill in the area between the
splint bone and the cannon bone, making it stronger and able to withstand the
strain. This may leave a hard knot that is not sore or inflamed and this is
also referred to as a splint , but technically would
be called a dead (healed) splint as opposed to a green (fresh or acute and
sore) splint. Refer to lower leg therapies for treatment protocols.
Fracture of splint
bones
Occasionally the ends of the splint bones ( the lower inch or so) will break off or fracture. This
will cause a mild lameness initially, along with signs of inflammation (heat,
pain and swelling). These can be diagnosed by x-ray and the veterinarian will
normally recommend they be removed surgically. This is not a major surgery and
the horse will usually be able to return to training within a week or so. If
they are not surgically removed, a calcium bump usually forms in the area of
the fracture and may only slightly bother the horse, usually not causing a
noticeable lameness.
Bowed Tendon
The back of the cannon bone anatomy consists of the
superficial and deep flexor tendon, as well as the suspensory ligament and the
inferior check ligament. When the Superficial and/or deep flexor tendon is
strained or sprained or sometimes even ruptured due to excess stretching, we
refer to the swelling in this area as a bowed tendon. Bowed tendons can be mild
to severe and involve a small area or a very large area. They are usually
caused by excessive stretching of the superficial and/or deep flexor oftentimes
because of tendon fatigue coupled with continuous work.
Initially this is an acute injury with all the
signs of inflammation (heat, pain and swelling) and should be treated as an
emergency. (Refer to lower leg therapies). Depending on the amount of
involvement of the tendons, the horse usually needs from 3 to 12 months rest
for healing to occur. If there has been a substantial amount of tendon fibers
involved in the injury, the tendon usually heals with much scar tissue and the
horse is left with a larger, thicker tendon area (bowed tendon). This healed
tendon would be referred to as a chronic bowed tendon. The tendon is never as
strong or resistant to stretching as it once was, and is prone to re-injury
more easily, although with controlled training and exercise, many horses with
chronic bows can be very useful for certain endeavors.
Suspensory Ligament Desmitis (desmitis refers to
inflammation of a ligament)
This injury would be very similar to the bowed
tendon, in that the fibers of the suspensory ligament have undergone excessive
strain or sprain or rupture. A ligament has less ability to stretch than a
tendon, so it can be more easily injured with overstretching. The suspensory
ligament is found beneath the flexor tendons, just behind the cannon bone, and
attaches to the top of the sesamoid bones. It can be injured anywhere along its
length. Refer to lower limb therapies for treatment protocols.
Check Ligament Desmitis
(inferior check ligament)
This is an inflammatory
condition caused by a strain or sprain to the inferior check ligament which is
located directly behind the cannon bone in the upper part of the cannon bone.
It is between the cannon bone and the deep flexor tendon. This can be a difficult
problem to find because it is deep in this area.

Conditions and lameness from the fetlock (ankle) down to
the hoof all are associated with excessive concussion causing an inflammatory
process in the area of involvement. These conditions can be aggravated by poor
conformation causing excessive concussive forces in a certain area of the
anatomy. The following is a summary of the conditions and the anatomical area
of involvement. Keep in mind that the conditions discussed from below the knee
down to the hoof are normally seen in the front limbs, and are not seen as
often involving the lower structures of the hind limbs. As stated earlier, this is due to the fact
the front limbs carry 65 –70% of the weight of the horse and therefore absorb
the most concussion. All of the conditions below will be helped by referring to
lower leg therapies and anti-inflammatory treatments.
Osselets – refers to inflammatory changes occurring over the dorsal
and lateral and medial areas of the fetlock due to excessive strain.
Sesamoiditis – refers to inflammatory changes in and around the proximal
sesamoids due to excessive strain of the area.
Ringbone – Calcification
or new bone growth on the first, second, or third phalanx caused by excessive
strain or injury to this area. High ringbone refers to P1 or upper P2, Low
ringbone refers to lower P2 and/or upper P3. Articular ringbone refers to new
bone growth within the articulation (joint) whereas non-articular ringbone
refers to new bone growth not involving the joint surfaces.